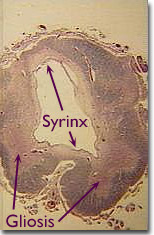
Syringomelia is a rare (prevalence
8/100,000) chronic, progressive degenerative condition in which a tubular
cavitation, called a syrinx (see MRI image, below left), develops
within the central parenchyma of the spinal cord (below right). Although the
syrinx usually develops in the lower cervical region, it may extend downwards
in the thoracic or lumbar regions, or upwards into the medulla oblongata and
pons (syringobulbia).

Almost 90% of syrinxes are
associated with congenital Type 1 Arnold-Chiari
Malformation, while an acquired syrinx may develop subsequent to
spinal cord trauma,
spinal arachnoiditis, and intramedullary cord tumours
(astrocytoma, hemangioblastoma, ependymoma).
- Disease
progression and clinical correlates:
- Highly
variable, depends on extent of syrinx and rate of its expansion
- Typically
insidious onset (average age: 30) with irregular intermittent progression
to wheel-chair bound state after 5 to 10 years
- Expanding
syrinx initially causes transverse enlargement of cord and compression
of neighbouring neurons and tracts
- Decussating
fibers in the anterior white commissure, carrying pain and temperature
sensation to the ascending
lateral
spinothalamic tracts,are
destroyed at the level of the syrinx, while uncrossed, rostrally-coursing
fine (discriminative) touch and proprioceptive fibers remain undamaged
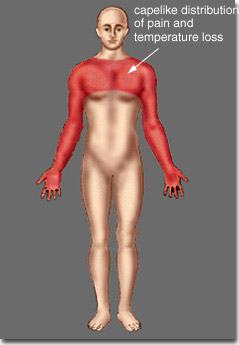
(below). This is clinically correlated by segmental dissociated
anesthesia,
the classic sign of syringomelia: pain and temperature sensation is lost
over a cape-like area, while discriminative touch sensation and proprioception
are preserved (below).
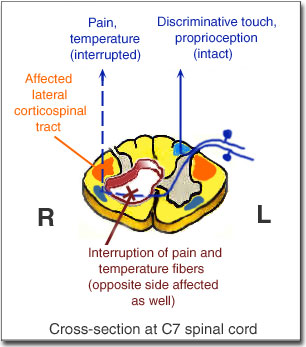
- Upon
syrinx expansion into the right anterior horn (above), destruction of
anterior horn cells leads right upper limb LMN symptoms and signs: motor
weakness and atrophy, fasciculations, loss of arm muscle stretch reflexes.
Associated conditions such as kyphoscoliosis (due to paraspinal muscle
weakness) may develop
- Expansion
of the syrinx into the right lateral corticospinal
tract (above) results in increased deep tendon reflexes and spasticity
in the right lower limb
- Late
symptoms include bowel and bladder dysfunction
- Deep
aching pain in neck, shoulders, or radicular pattern of arm and trunk
may occur early in the disease course
- Diagnostic
imaging:
- Myelography
- widened cervical cord, eroded pedicles
- CT
- repeat scan done after a metrizamide injection into spinal cord concentrates
in syrinx, revealing either expanded or collapsed cord
- MRI
- fluid-filled syrinx distinguished from intramedullary tumour